I like how they aren't saying Semaglutide in the title in an attempt to perhaps keep it from immediate scrutiny.
replies(3):
There are very complex dietary regimes that can be followed to minimize this, but most studies have shown that they don't save any time compared to losing weight and then working to get the muscle back afterwards.
> Dyck’s study comes on the heels of a commentary published in the November issue of The Lancet by an international team of researchers from the U of A, McMaster and Louisiana State University who examined emerging research showing that up to 40 per cent of the weight lost by people using weight-loss drugs is actually muscle.
This is, again 100% typical of what happens with caloric restriction.
That's the sort of headlines that smells like bullshit to me.
My understand of those drugs is that they don't actually make you lose weight, they just cut your appetite so you can follow a diet to lose weight without hunger hammering at the door. So to start with, if that's the case, all they are observing is the effect of a diet. Not sure the diet drug has much to do with it.
Then I went from 133kg to 88kg with these diet drugs. Even though I exercised every day, I am sure I also lost some muscle mass as well, just because I don't have to carry 45kg every time I make a move anymore. Seems logical and would probably be concerned if it was any other way.
>Studies suggest muscle loss with these medications (as indicated by decreases in fat-free mass [FFM]) ranges from 25% to 39% of the total weight lost over 36–72 weeks. This substantial muscle loss can be largely attributed to the magnitude of weight loss, rather than by an independent effect of GLP-1 receptor agonists, although this hypothesis must be tested. By comparison, non-pharmacological caloric restriction studies with smaller magnitudes of weight loss result in 10–30% FFM losses.
Comparing weight loss of different magnitudes is kind of comparing apples to oranges. Of course, it's not really possible to get persistent, large magnitude weight loss any other way than by using these drugs, so I understand why the comparison was made.
Without a control group who also ate the same amount of calories but without the drug, it's hard to know if the side effect were directly caused by semaglutide or just a result of being in a calorie deficit.
The only reason I want to lose weight is to eat more freely, won't be useful if I lose my appetite too.
I had multiple full body dexascans during the programme.
I didn’t change my exercise routine at all. I wasn’t hitting the gym or doing weights, just my usual basic cardio.
And I gained muscle and lost ~10kilos in weight.
It wasn’t much muscle, but the amount of muscle was higher than before.
For all of medical science's experience and history with debugging the human body, there's still so much more to understand.
The appetite comes back when you cut the meds, but it's an appetite based on your new weight. But if you then go on a some suggar rampage, you will regain weight and your appetite will grow too.
Those drugs are merely a guard rail to complete a diet successfully, but if people do not change their eating habbits, the same causes will produce the same effects after they cut the meds.
> Carla Prado, a nutrition researcher in the Faculty of Agricultural, Life & Environmental Sciences and lead author on the commentary, explains this rate of muscle decline is significantly higher than what is typically observed with calorie-reduced diets or normal aging and could lead to a host of long-term health issues — including decreased immunity, increased risk of infections and poor wound healing.
The rather obvious problem is that these GLP1 agonists don't improve your diet. If you continue to eat a protein and nutrient deficient diet (which is probably a majority of Americans) with caloric restriction on top of that, that leads to excessive muscle loss that you wouldn't see in a weight loss diet. This normally doesn't happen without GLP1 agonists, because these diets are too difficult to stick to for most people. Those who stick to them usually turn to nutritious high satiety whole foods that help combat the negative effects of caloric restriction.
Losing weight without losing muscle mass is very hard. It requires extreme diets like a protein sparring modified fast where 80%+ of your calories are from lean protein while running a 50% caloric deficit. If this research is correct, then using GLP1 agonists shortcuts the feedback loops that make the diets hard to stick to, but they shift the tradeoffs from weight to overall nutrition.
"When a measure becomes a target, it ceases to be a good measure" and all that.
https://www.sciencedirect.com/science/article/pii/S2452302X2...
This study on mice was suggested by a previous publication:
https://www.thelancet.com/journals/landia/article/PIIS2213-8...
where it had been noticed that in humans "the muscle loss with these medications (as indicated by decreases in fat-free mass [FFM]) ranges from 25% to 39% of the total weight lost over 36–72 weeks", in comparison with muscle loss of only 10% to 30% when the weight is lost just by eating less, without semaglutide.
So with semaglutide, a larger fraction of the weight loss affects muscles than when the same weight is lost by traditional means.
While for other muscles the loss of mass may not be so important, the fact that at least in mice the loss also affects the heart is worrisome and it certainly warrants further studies.
> Carla Prado, a nutrition researcher in the Faculty of Agricultural, Life & Environmental Sciences and lead author on the commentary, explains this rate of muscle decline is significantly higher than what is typically observed with calorie-reduced diets or normal aging and could lead to a host of long-term health issues — including decreased immunity, increased risk of infections and poor wound healing.
Do you have a source that 40% muscle loss is typical for a caloric restriction diet without GLP1 agonists?
MRI is the gold standard, everything else is pretty loosely goosey.
Sorry, no references but this comes up pretty often in the science based lifting communities on Reddit and YouTube if you want to learn more.
Maybe the mouse dose is just absurdly high? "Mice were then administered semaglutide 120 μg/kg/d for 21 days." That could be vaguely reasonable -- human doses range from, idk, ~36 to ~200 μg/kg/d (2.5mg/week to 15mg/week at ~100kg).
So if you have hypertension, this might actually be a "good" side-effect?
Emphasis my own. In short: no evidence this is anything other than due to rapid weight-loss.
As you point out, losing muscle is common in a diet, and the researchers are well aware of it. Their point was that this aspect is not pushed enough and is drowned by the losing weight part.
From the paper:
> Dismissing the importance of muscle loss can create a disconnect between patients' increased awareness of muscle and the role it plays in health, and clinicians who downplay these concerns, affecting adherence to and the development of optimised treatment plans.
[0] https://journals.lww.com/acsm-csmr/Fulltext/2019/08000/Effec...
For the "Fitness Versus Fatness" part for instance
I was with you up to here. In my experience it's easy to maintain a huge proportion of your lean tissue during a weight loss diet: Do some resistance training, get some protein, and don't lose weight too quickly.
There's no need to go to the extreme of a PSMF - which will still have you lose a bunch of muscle on account of being too big a deficit. If you can keep your calories reasonable while on a GLP1 agonist, there doesn't seem to be any reason you'll lose an exaggerated amount of muscle.
At least at a societal level, some increased rates of pancreatitis and a little suboptimal muscle loss are peanuts compared to what high obesity rates do to people at scale.
You're asking folks to make three separate changes: start exercising, change their diet to add protein, and use GLP1s to reduce food amount. And reducing food amount already goes against adding protein, so whatever protein they were getting is going to get cut even further.
> Together these data indicate that the reduction in cardiac size induced by semaglutide occurs independent of weight loss.
Which does sound concerning. It's the drug, not the weight loss, that causes the muscle loss.
I guess the question is whether it's better than nothing. Is the loss in lean muscle a worse outcome than remaining obese?
My understanding from initial anecdotes is this is actually literally wrong. Which was surprising to me, too. But people on GLPs tend to prefer more nutritious food (high protein and high fiber). I'm not sure if this has been studied directly in clinical trials yet but I know that food manufacturers have been reorienting their products toward healthier meal configurations in response to the GLPs.
I predicted the exact opposite of this, but so far I appear to have been wrong.
Yes it is.
> It requires extreme diets like a protein sparring modified fast where 80%+ of your calories are from lean protein while running a 50% caloric deficit.
I’m not any sort of expert but that sounds frankly, dangerous. I don’t see how you do something like that without damaging your liver.
It’s very possible to lose weight and gain muscle, but you have to be at just the right body composition (not lean and not obese) and then there’s a question of “over what period of time”?
Any duration under a month is probably pointless to measure unless you have some special equipment. Any duration over a month and it’s kind of obvious that it is possible. Eat a balanced diet without junk, work out regularly, and keep the calories to only what is necessary.
Beyond specific diseases we understand, it's still mostly a total mystery why we aren't immortal- we have not yet identified what is the basic mechanism of aging, or why it happens at different rates in different species, and mostly our systems are fundamentally capable of repairing and regenerating almost anything, but for some reason get worse and worse at doing so over time. Moreover, this doesn't seem to happen in all organisms- there are many animals that live ~4x human lifespans, and at least one species of jellyfish that is biologically immortal.
I bet there’s a large group of people - possibly over represented on HN and other online communities - that just need a little nudge to suppress their cravings and eat healthier, but that’s far from universal. For a lot of people, they wouldn’t even know where to start to eat healthier except choosing a salad over a burger at the takeout menu. Even with drugs masking cravings, many people just haven’t had good health or culinary education.
For most people, it just doesn't really matter, because their strength is so far below their peak capability it won't be hard to cut some weight while maintaining strength. The closer you get to the edge of capabilities, though, the more it will matter.
Is it possible to go very slow and keep most of your lean muscle mass? Sure. Is it practical? I have my doubts.
Part of the effectiveness of these drugs - for me at least - is that results are rapid and that is a self-reinforcing feedback loop. Diets that had me losing 1lb/week were simply too boring and unmotivating for me to keep up beyond a few months. A few days of vacation “cheating” and you wipe out a month or more of incredibly difficult to achieve loss. Restricting yourself mentally in what you eat every day adds up to exhaustion over time.
Some folks can manage to lose very slowly while also adhering to a strict calorie deficit of a few hundred per day, while also being consistent with resistance training. I’d say the evidence shows that these folks are in the small minority.
I will say more evidence is needed for this drug class - especially where the harm reduction principle may be a bit iffy outside of obese folks. However it was life changing to me in the way it let me change my eating habits to very healthy protein and veggies as my primary calorie intake, as well as made going to the gym on a strict schedule motivating enough to actually come out at the end with a better bodyfat to lean muscle ratio than where I started.
These gains have continued since I hit my goal weight - and now I’m starting to become one of those folks who the BMI no longer applies to in a good way. I do wish there was a good way to test heart muscle mass like there is lean body mass with a DEXA scan as I’m curious if my increased regular workout heartrates translates into building back any heart muscle mass like it did other lean muscle. Certainly a concern to keep an eye out for!
I’m curious as you are if folks who are slow responders and live active lifestyles see the same muscle loss the hyper responders do. For reference I lost over 100lbs in just under 9mo. I absolutely lost considerable muscle mass, but have since put it back on and then some.
So this isn't really 3 separate unrelated changes. Also at least in my experience, people tend to regard high protein things as the "energy dense" part of a meal - the problem with a lot of carbohydrates is they're not very filling.
The biggest problem with exercise is it's an awful way to lose weight - you don't burn that many calories, it makes you hungrier, and then your body optimizes to burn even less calories as you do it.
I did an InBody scan the day I started (8/21) and just happened to have done my second one this morning.
But if you're already lean and then go on a calorie deficit (as a result of decreased appetite from taking the drug), then muscle mass will be lost through metabolism of muscle and other tissue.
Then the study states further that the proportion of muscle loss is higher than expected from calorie restriction alone.
My gut feeling here is that where there's smoke there's fire, and I predict dramatic class action 40 years in the making, either like tobacco, or like baby powder, depending on the actual long term health outcomes.
And, this is great research! We need more like this ASAP!
> nutrient deficient diet (which is probably a majority of Americans)
First hit is some blogspam trying to sell me "Nutrient Therapy". Second hit is CDC: https://www.cdc.gov/nutrition-report/media/2nd-nutrition-rep...
> The Second Nutrition Report found less than 10% of the U.S. population had nutrition deficiencies for selected indicators.
I started losing weight from severe obesity with a caloric deficit but noticed I was also feeling weaker in general (aside from the tiredness that comes with eating under your TDEE).
I started going to a trainer and he had me change my macros so that I was consuming about 200g of protein per day in addition to 4 days per week of full body workouts on top of my cardio.
Since then I’ve lost an additional 150% of my initial weight loss, and have gained moderate muscle mass on top of that.
It doesn't mean they end up with the correct findings, but they are absolutely incentivized to try to produce correct findings.
Lazy and inapplicable heuristics are not legitimate insights.
While acknowledging that the mechanism is different, this was the same effect of Ephedrine, which went through a similar craze as Ozempic before the full complications were known. My bet is that this will be similar, where the risks end up being outweighed by the benefit for extreme obesity and diabetics, but that the cosmetic weight loss aspect of it will become outlawed or highly regulated.
> Losing weight without losing muscle mass is very hard.
What is the current comment receiving most of the comment?
"That's the sort of headlines that smells like bullshit to me"
That's the sort of comment that smells like bullshit to me. What kind of place is this?
Many times I find the posts on HN interesting, but increasingly these kind of comments make me wonder about Y Combinator. Is this really the best they can do?
And for us readers who are supposed to be so called hackers, is this the best we can do?
I’ve understood that generalizing anything in today’s time is a losing game. I know many people with IBS/GI issues and I am also sure they have different underlying causes. Our gut biome and how digestion works in general needs to be researched much more.
I don’t know why progress has generally been so slowly on that front. For instance, GLP-1 was discovered in the 1970s. It took us another 40 years to commercialize it in the form of Semaglutide and another 10 years to get it ready for human consumption.
Is it true the majority of Americans eat a protein deficient diet? I always thought there was too much protein in the western diet - nearly at every meals versus how we would have evolved with somewhat limited access.
I was under the impression that consumers have been asking for healthier food compositions for decades, probably since the 70s or 80s when all the FUD around fat started. Maybe GLP1 agonists bring their buying choices more inline with the focus group results which would be an interesting phenomenon.
Their hearts are not physically smaller, nor did they shrink during their build-up to current physique.
Saying things like this is harmful at best. Please don’t.
> It's a bit difficult to add more weight lifting because I tended to hurt myself
> with no medical care [...] something no computer or man made complex machine comes close to.
That's because we get far more units of "work" out of our machines than the person living for 70 years with "no medical care." Some people live just 30 years with no medical care too. And the machine does not need to sleep. We eat food they eat lubrication oil. I don't think this was a good analogy.
> it's still mostly a total mystery why we aren't immortal
While we haven't pinpointed the mechanism, we have a pretty good idea of why, and where in the system we should be looking for the answers.
> but for some reason get worse and worse at doing so over time.
You are a living Ship of Theseus and these "error correction" mechanisms are not perfect. Aside from this there are known genetic disorders which alter the rate at which people age. This is not nearly as mysterious as you're making it out to be.
> there are many animals that live ~4x human lifespans
And what are their resting respiration rates?
> and at least one species of jellyfish that is biologically immortal.
In theory. We haven't found an immortal one yet. They all die. They're also nowhere near our level of biological complexity or capability.
I haven’t seen any credible research that a healthy person can damage their liver from excessive protein intake. Someone suffering from liver disease needs to be careful, sure, but evidence that it would harm a healthy liver is practically nonexistent.
That said, PSMF is explicitly not a sustainable diet and proponents generally don’t claim it to be. It’s a short term diet meant to preserve muscle mass under extreme caloric restriction (under 1.2k calories).
> Eat a balanced diet without junk, work out regularly, and keep the calories to only what is necessary.
If it were as simple as that, we wouldn’t be having this conversation.
And I don't eat meat for non-dietary reasons that include existential risks to all of humanity:
- Pandemics - Where did the "Spanish" flu (and influenza A, Asian flu, HK flu, and 2009 pandemics) and COVID come from?
- Antibiotic resistance - Most classes of antibiotics used in humans are also used to make industrially-farmed animals grow faster, leading to greater antibiotic resistance and more potential bacterial pandemics too
- Climate change - 17%, at least
- Air pollution - Not just the smell of pig crap in the air
- Water pollution - Ag runoff has been ruining river delta systems
- Soil pollution - (It's gross)
- Fewer available calories for total consumption
- More expensive foods by less supply and more demand
(Never bother with "meat is murder" dramatic preaching because most people who eat meat suffer from cognitive dissonance preventing them from admitting their lifestyle choice causes animal cruelty.)
When I was on and could afford semaglutide, I improved my diet by consuming a high protein product with a low calorie breakfast nutrition supplement. I'm sure I probably could've accomplished similar with a multivitamin and a protein product. What I need to change is eating more low calorie, high fiber fruits and vegetables that don't taste like cardboard or a mowed lawn. My diet has gone to shit again because the insatiable, all-consuming (no pun intended) hunger has returned. I can't afford semaglutide right now so I must become unhealtier than simply obesity in a similar but lesser way than women who can't get surgeries until they're septic and dying from failed ectopic pregnancies before it will be covered... because somehow obesity is completely my lack of willpower when I wasn't obese before mirtazapine.
This makes sense. If fasting hurt your heart many of your ancestors would have died early. There is strong selection pressure to survive extended fasts.
For purely technical topics you expect good quality discussion, but those threads barely get comments in the two digits.
Also, "just do proper resistance training" is a bit of a stretch when we're talking about what is practical to expect of the masses taking Ozempic.
Most people should mainly be eating fat and protein with a decent amount of grains and fruit and vegetables. However, the standard advice is to eat a lot of grains, some fruit and vegetables, a modest amount of protein, and little fat. This is awful and leads to very high hunger. Especially if you eat multiple meals a day, as is also commonly recommended, this is a recipe for being ever hungrier day by day.
It wasn't until I eschewed all advice, started eating one big meal a day and maybe one snack and matching my carb intake with my fat intake that the hunger that I had known since childhood magically disappeared and I lost 25 lbs (and am losing more). Finally a 'normal' weight seems not only in sight, but extremely easy!
It pretty much is that simple. The problem is that simple is not easy.
I also think it’s a symptom that HN does not allow enough people to use the down vote button. you could be a commenting member for years and not be able to downvote or you could be somebody who posts a few click bate links you copied from another aggregator and all of a sudden you have the ability to downvote. It’s pretty dumb.
Nope, not a problem. I just get full much faster and am even more prone to simply not eating when I’m busy, than I already was. Not as food-focused when idle, but I still snack a little or whatever.
> emerging research showing that up to 40 per cent of the weight lost by people using weight-loss drugs is actually muscle
Which is… obviously bullshit.
Not only that but prescribers and patients have noticed that GLP-1 agonists also appear to significantly reduce people's consumption of drugs like alcohol, nicotine and opioids. At least in some populations.
Much more research is needed but right now it's extremely promising that they will have a place in addiction treatment in the future.
HN is the only forum I know of that has broadly grasped that most so-called “science” outside of the hard sciences and mathematics is complete garbage and driven by funding needs. The world is awash in non-knowledge. This is an extremely serious issue.
Building the skill to rapidly come to a preliminarily judgement of a headline is crucial.
For me, that hasn't even been the case. I'm down 40lbs on a relatively low dose of Semaglutide and my muscle mass has moderately increased over the last 6 months. The hysteria over this is totally unfounded.
Um, when your appetite is "crushed", nothing is particularly appetizing. That is the entire point. It allows one to make better decisions or pass on eating.
My friend cut usage after he lost weight and finds maintenance easy.
I can't read the original sources there, but what makes you say its obviously bullshit?
To your point, the drug is absolutely to do with it if by taking the drug people need to be more mindful of the types of food they eat, if they have a smaller window to consume nutrients.
It is most certainly a contributor and for some who may not exercise like you, or consume an appropriate level of protein this research may show that those taking the drug need to focus on a more protein right diet.
It's been years since I've had that mindset when entering any thread above a certain number of comments.
Remember in the 80's and 90's when exercising and being healthy was considered a cool thing? Remember there was a gym on every corner and people were all about looking good and being healthy, eating healthy and living longer?
Then somewhere. . .
- We started normalizing obesity.
- We started this whole "body positivity" trend that celebrating morbidly obese people like Lizzo as positive role models was a good thing?
- We started introducing fat mannequin models in retail stores because being obese shouldn't have a stigma?
Obesity is a problem because we, as a culture have completely normalized obesity. Instead of promoting healthy diets and exercises and saying being obese has consequences like shortening your life and will make you susceptible to various diseases like diabetes and heart disease? All we've done is told people its ok to be obese and eat sugary drinks and over processed foods, because you can just have surgery and that will fix it. Or you can take a pill and that will fix it.
IT WON'T.
IT NEVER WILL.
We've gone down a road that is staggeringly dangerous because we've accepted being morbidly obese as something that's completely normal.
My take it this.
The median scientific paper is wrong. I wrote a wrong paper. The average biomedical paper doesn't fit the standards of the Cochrane Library mostly because N=5 when you need more like N=500 to have a significant result. Since inflationary cosmology fundamental physics has been obsessed with ideas that might not even be wrong.
It's well known that if you lose a lot of weight through diet (and even exercise) you are likely to lose muscle mass. With heavy resistance exercise you might at best reduce your muscle loss if you don't use anabolic steroids and similar drugs. That you could have changes in heart muscle with using these weight loss drugs isn't surprising for me at all and it's the sort of thing that people should be doing research both in the lab and based on the patient experience.
(Funny you can get in trouble if you do too much exercise, spend 20 years training for Marathons and you might get A-Fib because you grew too much heart muscle instead of too little.)
A lot of the cultural problem now is that people are expecting science to play a role similar to religion. When it came to the pandemic I'd say scientists were doing they best they could to understand the situation but they frequently came to conclusions that later got revised because... That's how science works. People would like some emotionally satisfying answer (to them) that makes their enemies shut up. But science doesn't work that way.
The one thing I am sure of is that you'll read something else in 10 years. That is how science works.
All I can say is try losing 20 pounds and keeping it off for two years and how easy it is. Fat shaming might make a difference but I suspect it would be like knocking off 5 lbs from the average where you really need to knock off 50 lbs.
You only started seeing Victoria's Secret getting fat models in the last few years, the obesity epidemic on the other hand started in the Regan years. Maybe it's like taking your belt off when you get heartburn (though I know if I go that route pretty soon I'm going to need suspenders) Try
https://arxiv.org/abs/q-bio/0312011
for a theory that may be wrong but fits the chronology.
Yes, I am trying to hit 100-150g+ of protein per day, yes I am in a caloric deficit. No, I don't feel like I have lost any muscle mass, but I do feel a lot more active at 60lbs lighter.
Semaglutide is based on a 31-amino acid polypeptide that mimics the human GLP-1 hormone. At position 26, the lysine side chain is conjugated with a fatty diacid chain, to slow degradation and prolongs half-life, and there are some other modifications. However, the target - the GLP receptor - is not just expressed in the intestinal tract but all through the body, in muscle, central nervous system, immune system, kidneys and others. So some unexpected effects beyond the desired ones are likely.
Semaglutide was recently shown to have potent effects on the heart, and possibly beneficial to certain heart disease conditions associated with obesity. Makes me suspect this drug should be restricted to clinically obese cases where strong intervention with close medical supervision is needed. However for healthy people who just want to lose a relatively small amount of weight it really doesn't seem wise.
"Semaglutide ameliorates cardiac remodeling in male mice by optimizing energy substrate utilization..." (June 2024)
Did you read the paper or skim its abstract, figures, and conclusion? I'm not so sure that commenter did, or they may have cited this,
> Because we report smaller cardiomyocytes in cultured cells and in mice treated with semaglutide, it is tempting to speculate that semaglutide may induce cardiac atrophy. However, we do not observe any changes in recognized markers of atrophy such as Murf1 and Atrogin-1. Thus, we cannot be certain that semaglutide induces atrophy per se or if it does, it may occur via molecular pathways that have not been identified herein.
> Building the skill to rapidly come to a preliminarily judgement of a headline is crucial.
You can't judge this paper based on the popsci headline.
> most so-called “science” outside of the hard sciences and mathematics is complete garbage and driven by funding needs
Based on my reading of the figures and conclusion, I don't think you should call this paper garbage.
People who promotes fat positivity are ridiculed.
Blaming it on culture overly simplify the issue, which is going to be a complex mix of interacting causes.
"Studies suggest muscle loss with these medications (as indicated by decreases in fat-free mass [FFM]) ranges from 25% to 39% of the total weight lost over 36–72 weeks. This substantial muscle loss can be largely attributed to the magnitude of weight loss, rather than by an independent effect of GLP-1 receptor agonists, although this hypothesis must be tested. By comparison, non-pharmacological caloric restriction studies with smaller magnitudes of weight loss result in 10–30% FFM losses."
The "surprising" part is kinda bullshit, and implies there's something special about glp-1s. It is the opposite of surprising that weight loss includes a lean mass loss.
That said, being skinnyfat is probably bad for you and the idea that you should work to preserve/build muscle and not only lose weight is a good one.
Your comment lacks any substantive argument about the comment you complain about.
Apparently the topic is “important”. To me an appeal to importance when policing style spells like bullshit.
I'm not an expert, but I have to imagine that most of it is muscle.
After dramatic weight loss, a person will probably lose some bone - particularly in the lower body - due to decreased loading.
I know body builders sometimes eat extremely high protein diets (more than 1 g/lbs of body weight) and lift quite hard to try to hang on to as much muscle mass as possible. And they still lose some when cutting.
Some of it is likely bone density as well. You can prevent the bone density and muscle loss with proper diet and exercise, though.
The modern weight-loss programs I'm seeing now (at least those aimed mostly at middle-aged men) emphasize consuming significant amounts of protein (2g for every 1kg of body weight each day) and engaging in regular resistance training, in order to maintain muscle mass.
The article addresses this:
To keep muscle strong while losing weight, Prado says it is essential to focus on two main things: nutrition and exercise. Proper nutrition means getting enough high-quality protein, essential vitamins and minerals, and other “muscle-building” nutrients. Sometimes, this can include protein supplements to make sure the body has what it needs.
Perhaps there needs to be more formal research into this, and a strong recommendation made to everyone using these drugs that this kind of diet and exercise plan is vital.
OK I actually checked up on this, and it is more like 30%, but that number gets worse as you get older. For young healthy men it can be 20%, but as you get older that number gets worse and worse.
I'd want to see a comparison of a similar cohort of people going on a calorie restricted diet of the same magnitude, with a similar (lack of) activity levels.
The study at https://www.thelancet.com/journals/landia/article/PIIS2213-8... compares people who had less overall weight loss on a pure calorie restricting diet, which, well, by definition isn't the same thing.
If you're doing resistance training for the first time in your life or the first time in years, noob gains will outpace loss if you train hard and get adequate protein. This is the case for a lot of people on these GLP-1s, at least at the start.
But if you have a massive quantity to lose, as in a multi-year process, you won't be able to keep up the noob gains for the entirety, and then yeah, you're going to basically just be training hard and shoving protein down your face just to keep the muscle loss minimal.
It's good to work out. Perhaps it offsets any loss.
I get that it's upsetting and might contradict what you think.
At this stage we don't know for sure. It's something you might want to keep in mind. Especially if you take this drug without working out.
Bodybuilders will even take AAS that explicitly reduce catabolism of muscle mass like Anavar and still lose some muscle on cuts.
Getting on tirzepatide made it trivially easy for me to get back to a better diet, start exercising, etc. I do have to force myself to have an extra protein shake to hit my macros, though.
Estimates in level of inaccuracy on the high end ranges from ~5% to ~10%
If you see your lean mass going up in DEXA, your muscles are getting larger, and you're getting stronger, particularly across a wide variety of exercises where CNS adaptation can't explain the strength gains, they're likely broadly accurate.
Mine have all tracked quite closely with what I'm seeing in the mirror and what is happening when it comes to the amount of weight I'm moving.
So why, after 20-years, and millions of people haven't fen-phen-like side effects appeared?
Also, concern of losing muscle mass on GLP-1 agonists (and diets in general) is well known and typically explained by the responsible MD to the patient.
It’s perfectly possible for a new hot to have a severe side effect that won’t be noticed for quite a long time.
Semiglutide appears to have undergone final clinical trials in the US around 2017. Given it hasn’t been on the market terribly long and has only an exploded in popularity relatively recently it doesn’t seem like it would be that hard for it to have a serious side effect in a small portion of the population that hadn’t been detected before due to the limited number of people taking it, the amount of time it takes to manifest, or both.
Obviously it’s providing significant benefit that risk could easily be worth it. But as it gets marketed towards more and more people that won’t be true for all of them.
The point is is that most people lose muscle because they’re not lifting. You will lose muscle if you lose weight no matter the cause, if you are not lifting weights.
"Specifically, we found that BMIs from 40 to 44 were associated with 6.5 years of life lost, but this increased to 8.9 for BMIs from 45 to 49, 9.8 for BMIs from 50 to 54, and 13.7 for BMIs from 55 to 59."
I think for some people the roi is measurable and reasonable.
https://irp.nih.gov/blog/post/2020/01/extreme-obesity-shaves...
This conversation does make me wonder about whether or not it would make sense to make the option available for people to go on exogenous testosterone (and yes potentially even women) while on these to help prevent muscle loss.
I don’t think it would have been possible to not lose substantial muscle mass while rapidly losing 100lbs over 9mo, even with extreme resistance training added to the mix. While DEXA scans are not super accurate, I’ve put on about 17lbs of muscle since my first scan 10mo ago, while maintaining a 12% or less bodyfat ratio.
That said, I’ve been eating extremely healthy both before and after being on the drug which helps a lot. The drug simply gave me the mental space to avoid the binges which were my particular problem. That and it controls portion sizes to European dinner vs. American restaurant sized meals for me.
I wouldn't blame anyone for choosing the drugs over dying early.
[1] https://www.healthline.com/health-news/obese-people-have-sli...
But as someone who spent a good chunk of their early adulthood having no problem with healthy habits and then slowly slipping into tons of bad ones, getting on tirzepatide has made it as easy for me to make those healthy choices that I made when I was in my 20s. Ones that I struggled with mightily after I got fat.
Hopefully more and more people will use them as a tool to help them get things back and order and then stay there, whether or not they keep taking it.
As these become more common and doctors more aware, the dosing guidelines will become much more nuanced and dialed in.
I assume you mean gastroparesis - this is an extremely rare side effect
> Bad depression
Again, pretty rare side effect.
If you think these are the minor things I'm confused as to what you think the major side effects are.
My DEXA scans seem roughly correlated with the amount of weight I can do in my regular sets, which has increased about 50-70% depending on which muscle group you are talking about.
This is with heavy resistance training 3 times a week and Pilates once a week.
If it was "killing people", we would be seeing it literally everywhere. We're not talking about a small scale 50K+ observation... we're talking about literal millions.
I was 92kg when I started on liraglutide (I was doing GLP-1 agonists before it was cool!) and 67% of muscle mass (61kg). I'm now at 69kg and 82% of muscle mass (56kg). I'm doing weight and resistance training twice a week, in addition to aerobic training.
One nice thing, while muscles don't become more massive, they for sure become more pronounced and visible with weight loss.
My experience matches at least a dozen folks in my personal bubble. It’s sort of the point of the drug or it wouldn’t work very well.
Totally agreed on resistance training. The one thing I would change would have been starting that in a serious manner as soon I started the drug vs. waiting. Prescribing it is silly though - if that worked we wouldn’t need the drugs to begin with.
Looking through my weightlifting app my best tracked exercise (leg press) increased about 250% from start with a 60% (roughly, speaking from memory) increase in lean muscle mass as measured by a DEXA scan. If I remember when back from dog walks tonight I’ll update that with a real number off the actual data.
I was a total newb at lifting though, so those early gains came quite quickly.
I am curious as this is a concern I have for long term health.
https://amp.cnn.com/cnn/2024/05/10/health/ozempic-glp-1-surv...
Maybe you can titrate off the drug and in a perfect world, the hunger signal doesn't come back on all the time; that'd be great. Maybe, while on the drug, you've developed eating habits that you can continue while off the drug, even though you feel hungry all the time, again. Maybe, it's just too hard to ignore the hunger signal, and you need the drug for a lifetime.
That's not to say these drugs are necessarily wonderful. Previous generations of weight loss drugs came with nasty side effects that weren't immediately apparent. Fen-Phen was a wonder drug until it ruined people's heart valves. Stimulant appetite supressants have issues because they're stimulants. Cigarrettes have appetite supressant properties (not surprising, nicotine is a stimulant), but they're cigarettes.
Personally, I don't have an overactive hunger signal; so when I eat poorly and gain weight, it's on me. But other people I know have a totally different experience with hunger. If your body is telling you all the time that you need to eat, it's hard to say no. Just like it's hard not to scratch when your skin is itchy. I can resist itchyness sometimes, but when it's constant, I'm going to scratch.
Professional body builders do bulk/cut/bulk/cut because after awhile you can't lose weight and put on muscle at the same time, especially if you want to get to the point of being shredded.
(well you can do it, but there is no benefit over bulking and cutting)
Second gotcha: how much of the decrease is just attributed to the lower mass of the subject after the weigh-loss treatment
Though it's one good reminder that "catabolism" and "anabolism" are less selective than we wished to
I just think the level of effort involved is different. For instance, the person who posted the link to the study we're now discussing earned 199 points with far less effort than you put into replying to my comment. Many of the links posted are copied from Reddit, Twitter, Slashdot, etc.
Vanishingly few people succeed in exercising discipline and self-control long term. But obesity is caused by food addiction and the idea is once you've kicked the addiction and got over the withdrawal etc then it's gone and you no longer have to fight it. I don't "exercise discipline" to stay thin. I just don't eat copious amounts of junk food because I'm not addicted to it.
So if the drugs are used to soften the withdrawal symptoms such that people can learn to like real food and kick the addictive crap then that's good. But if they're used as a magic pill with no other lifestyle changes then I'm sure people will just go back to what they were doing before once those pangs come back.
I'd still rather we went after the industry peddling the addictive shit. We went after the cigarette companies. But food companies seem untouchable.
Vaccines and antibiotics and germ theory are all things that seem “too good to be true” but nevertheless are. Should we be worried that clean fusion power, once commercialized and practical, is going to somehow cause some catastrophic unknown future event just because it yields immeasurable benefit to us?
I think this is just another form of magical thinking.
It's the same with e.g. human growth hormones, one theory is that Elon Musk is / has used them, but without the weight training that should go with it, so his body has developed really weirdly.
With exercise, the heart muscles grow in a different way, and the volume of blood contained inside is not reduced. So without looking at the heart itself, we can't even tell whether a lot of muscle is good or bad, we also need to look at the rest of the context.
My wife told me exactly this - potentially all muscle mass loss (and she made sure I understood that 'all' part), yoyo effect once stopping, potentially other nasty long term/permanent side effects, and overall just a bad idea, attacking the problem from a very wrong direction. Just look at musk for example - he pumps himself with it obsessively and the results even for richest of this world are... not much there (or maybe his OCD binging would make him 200kg otherwise so this is actually some success).
Then all the folks come who say how to helped them kickstart a positive change, like its something against those facts above. All the power to you, just don't ignore facts out there and don't let emotions steer your decisions. You only have 1 health and it doesn't recharge that much, and that short time we have on this pale blue dot is significantly more miserable and shorter with badly damaged health.
The modern weight loss program you described is pushed because that's what people want; an extremely low-effort methodology that yields extremely high results.
The idea that their is some silver bullet to weight loss has dominated the US health market for ages now because selling someone a pill that they don't have to do anything but swallow and be cured is really, really easy.
Having gone through my own weight loss journey, I have seen first hand how attractive that is and fell for it myself twice. So have loved ones, one whom is no longer the same person because they got gastric bypass which resulted in a massive change to gut and brain chemistry, something that we seem to be just figuring out is connected. My own journey is not over, but there are no longer any medications or supplements involved, because I can say with authority that none of them work without good nutrition and physical exercise.
As I realized this and just put more work into eating better and doing more activities (I did not join a gym, but started riding my bicycle more, walking neighbor's dogs, and doing body-weight exercises at home, etc, making it more integrated into my day rather than a separate event I could skip), I lost a healthy amount of weight and got stronger.
It took a lot longer, of course, than what the pills promised, but that's the trick of the whole weight loss industry...and make no mistake, it is an industry. Short-term results in exchange for your money. It was never about helping people be healthier and always about myopic profits, therefore we should not be trusting any claims these companies make that their silver bullet is the correct one, finally.
And yet.
I’ve seen multiple friends go from eating like shit, including chugging sodas, to not compulsively ordering dessert and no sodas in the house. I think all of them have since quit Ozempic, each seeing some rebound but nothing comprehensive and, most notably to your argument, not in the behaviour modifications.
This is a really stupid argument, your data point of "one friend" or even two or more friends with unspecified timeline is useless. The only thing that has any meaning is a formal study with a large number of participants over many years of observations.
Just like in programming, there is no silver bullet; there's only hard work.
There is suspicion that they had a pre-existing mental health issue they were hiding, and the very fast changes that happened in their body triggered it to either manifest or get worse. We are left guessing because they refuse to see any doctors that won't just write prescriptions for meds or minor elective surgeries, now.
These days, more and more evidence is piling up about the gut-brain connection, but no conclusions are being drawn quite yet. Though, from my own experience, it is not difficult to convince me that one certainly impacts the other.
At 40% muscle loss you're getting awful close to losing weight while increasing your body fat percent!
But of course you're right that diet+exercise is key but for those maintaining such, they wouldn't end up on these drugs to start with.
I think it's a mistake to think of it as what people want. It's what people can do.
We have to acknowledge a fundamental struggle that we have with dieting and working out. Pretending it's just hard, when statistics show what is true at a societal level, will not bring us solutions.
We need something else. Either that's massive societal change to i.e. approach something like the diet/workout culture you have in Japan. That's hard. Or, as with many other of our health problems that we can't just will away, it's drugs.
Not believing in progress here, when drugs progress everywhere, is unnecessary. Current generations might have issues. Drugs will be better. We won't.
Of course you do! If your body is tens of pounds lighter, then you don't need the extra muscle to lug it around. This paper is about reduction in heart muscle, and of course your heart doesn't need to be as strong because there's less blood to pump and less tissue to fuel.
When you gain weight, you also increase the muscles needed to carry that weight around. If you see someone obese at the gym doing the leg press, you may be astonished at how strong their legs are. When you lose weight, you don't need that muscle anymore.
Our bodies are really good at providing exactly the amount of muscle we need for our daily activities (provided we eat properly, i.e. sufficient protein), so it's entirely natural that our muscles decrease as we lose weight, the same way they increased when we gain weight. Muscles are expensive to keep around when we don't need them.
Obviously, if you exercise, then you'll keep the muscles you need for exercising.
But this notion that weight loss can somehow be a negative because you'll lose muscle too, I don't know where it came from. Yes you can lose muscle, but you never would have had that muscle in the first place if you hadn't been overweight -- so it's not something to worry about.
This isn’t a surprise unless people ignored reading about the drugs before taking it and ignored the doctors.
The study is actually a published letter [1], and it doesn't appear to account for this. Science Direct even published a study about this in 2017 [2]:
> Weight loss, achieved through a calorie-reduced diet, decreases both fat and fat-free (or lean body) mass. In persons with normal weight, the contribution of fat-free mass loss often exceeds 35% of total weight loss, and weight regain promotes relatively more fat gain.
We already know how to reduce the effect of this, the person simply needs to increase exercise as the weight is lost in order to maintain lean muscle mass.
[1] https://www.sciencedirect.com/science/article/pii/S2452302X2...
[2] https://www.sciencedirect.com/science/article/pii/S216183132...
https://jamanetwork.com/journals/jama/fullarticle/2810542
https://pmc.ncbi.nlm.nih.gov/articles/PMC10874596/
https://pubmed.ncbi.nlm.nih.gov/38443105/
Or more plainly worded
https://www.healthline.com/health-news/ozempic-wegovy-stomac...
Some people develop permanent gastroparesis.
You will still lose "muscle", and some of that will be in the fat embedded into the muscle.
I would recommend checking out some of the learnings from the keto diet. You may or may not subscribe to it, but they had to very carefully tread these lines when the body was essentially in starvation mode. A few things I know of:
1. You have to maintain a certain amount of protein intake (~10% to ~20%) to prevent your body burning lean muscle mass.
2. Too much protein gets converted into sugars, these in turn are easily stored as fats.
3. Maintain exercise, use it or lose it.
4. Don't over-exercise. "Exercise flu" results in limited performance and muscle loss through gluconeogenesis. You break down muscle and convert it to energy due to lack of carbohydrates.
https://www.minimumdosetraining.com/ - free training program + links to a bunch of studies the author was involved in on this specific subject.
However, a lot of people either see results on these initial doses, and plenty of people find them to be effective as maintenance doses.
HFCS consumption (along with added sugar consumption in general) peaked in 2000 and declined steadily until 2020: https://news.ycombinator.com/item?id=38094768
> Using mice for the study, the researchers found that heart muscle also decreased in both obese and lean mice. The systemic effect observed in mice was then confirmed in cultured human heart cells.
So it also happened for already lean mice (though no mention of whether they still lost fat), and for cultured human heart cells (so not a by-product of needing less muscle to pump blood through a shrunken body).
https://scholar.google.com/scholar?as_ylo=2024&q=glp+1+thyro...
It is not immediately clear if the muscle loss happens faster (probably) what the immediate impact of that is, and whether or not you lose more muscle mass on one or the other.
That is exactly the risk. Our bodies are really good at it. But we are taking drugs that may change what our bodies do. Even a small bit of extra heart muscle loss may push as below where our bodies would have left us naturally. Is that dangerous? Are there people who need to worry about it? How do we know whether or not that should be a concern? It raises questions, and is worthy of discussion, even if we do land at answers that say it is an acceptable level of risk.
Based on people who I know have been taking these drugs, they make it much easier to reduce calorie intake by promoting satiety. That’s the benefit.
Doing the rest of your life while you feel hungry is not fun, and willpower is not infinite.
People do no realize how wide spread the GLP1 receptors are in the human body. GLPL1R is expressed on all muscles so heart muscle will be effected:
https://pmc.ncbi.nlm.nih.gov/articles/PMC5939638/
https://www.proteinatlas.org/ENSG00000112164-GLP1R/tissue
The way these drugs help loose weight is by increasing cellular activity by stimulating adenylyl cyclase and increased intracellular cAMP levels. It is not that hard and not a msytery to anyone who can think straight about human metabolism.
The warning isn't that you're losing muscle during weight-loss with these drugs. It's that the ratio of muscle vs fat loss is much greater with the drugs compared to traditional weight loss methods.
It's been well studied that if you exercise and eat enough protein while losing weight, you can retain more muscle.
Losing a lot of lean mass is incredibly detrimental to your longevity and quality of life.
While true, its also true that if you manage to lose substantial fat in the process, it leads to longer and better quality life
I gained muscle, as I started weightlifting (modified 5x5 program 3-4 times a week) and was supplementing with protein isolate (about 50g a day).
My subjective feeling is that even if "Ozempic makes you lose muscle faster than the same caloric deficit without it" is true, this effect is very small.
Vast majority of muscle loss comes from no resistance exercise, low protein, much faster weight loss than possible "naturally".
The study on mice published in the second article has been made specifically to test this optimistic supposition and the results have shown that it had been false, i.e. the weight loss caused by semaglutide is different from the weight loss caused only by calorie restriction.
More studies are needed to elucidate whether this effect of semaglutide is really harmful or maybe it can be reversed or avoided by combining the medication with a better diet, e.g. with a higher protein intake.
https://www.liebertpub.com/doi/abs/10.1089/thy.2023.0530
> Overall there is no conclusive evidence of elevated thyroid cancer risk.
https://dom-pubs.onlinelibrary.wiley.com/doi/full/10.1111/do...
> Our meta-analysis showed that GLP-1RA treatment could be associated with a moderate increase in relative risk for thyroid cancer in clinical trials, with a small increase in absolute risk. Studies of longer duration are required to assess the clinical implications of this finding.
It's potentially a possibility, but the absolute risk seems to still be quite low.
It keeps happening because the market wills it to, but not without good reason. It is perfectly rational to want something to be easy, especially now as our modern lives are inundated with a tremendous amount of stressors and tasks we must constantly attend to. So yes, we wish for convenience, but it is not the solution we always need.
Skinny people move to the US and get fat. They're not skinnier back in their home country because they've got greater willpower or are harder workers, but because they aren't in the US. If harder work isn't why skinnier countries are skinnier, we shouldn't expect it to help us out of our problem, and indeed, we have nothing else we've studied that is terribly effective over time, and certainly nothing cheap enough to deploy on a large scale.
Again, yes, for an individual your perspective is the only thing one has (well... until these drugs) but looking from a policy level, it's useless.
It's a devious euphemism that screws the people over the most that should be eating more beans and broccoli (et al).
The problem is that the average joe's daily activity is incompatible with an healthy muscle mass. After 30 if you don't actively exercise you lose muscle mass, if you're obese, 50 and starve yourself or take drugs that make you lose more muscles than necessary you won't gain them back ever unless you do some form of serious resistance training
https://hips.hearstapps.com/hmg-prod/images/triathlete-aging...
These drugs are turning into a band-aid on the fact that it's more profitable to sell addictive, high-calorie foods in the US than foods that promote long-term health.
We'll decay people's heart muscles before we put a tax on unhealthy food to help fund Medicare and Medicaid.
Yeah, I've swung 10lbs in 24 hours just going from well fed to fasted without water. And it certainly wasn't fat I lost, just water and I'm surely any mass in my... various tracts.
It appears that they fed the control group and treatment group of mice lots of food to get them fat, then gave them identical normal diets, and gave the treatment group semaglutide.
The semaglutide group lost significantly more weight (fig A.ii) than the control group, and also lost heart muscle.
So it does not seem that they compared to an equivalent amount of weight loss in mice, which is what I'd think you'd need to do to come to the conclusion from the article (actually, not just an equivalent amount of weight loss, but also at the same rate).
[1] https://www.sciencedirect.com/science/article/pii/S2452302X2...
https://news.ycombinator.com/newsguidelines.html
If you care to actually have a conversation about the article, feel free to respond to some specifics I provided here:
Yes, you are right that DNA repair mechanisms are not technically error correction in the sense that the term is used in computer memory and storage, where any isolated error is mathematically guaranteed to be correctable. You clearly have a bio background, but my intent was to point out in a simplified way to non-bio people that biological systems do have mechanisms to deal with errors. I incorrectly assumed that you didn't have a bio background, and I can see that my message would have seemed a bit condescending- my apologies.
> While we haven't pinpointed the mechanism, we have a pretty good idea of why
I study metabolism and have observed things that aren’t compatible with any of the leading theories- which I suspect are all dead ends. We are definitely missing something big still. In particular, I feel like the big anti-aging startups are throwing good money after bad, by massively funding researchers with mostly played out dead end ideas. Tech billionaires funding this stuff are re-playing the same scenario as the ancient Chinese emperors and their mercury based elixirs of immortality in modern times IMO.
Hmm, that is not my experience generally. People will take insanely ineffective routes if that is what the system pushes them toward, without taking much offense.
For example, on the topic of health/weight loss: Weight Watchers or yoga classes are huge industries while also being insanely elaborate and expensive ways of eating better and moving your body.
I agree with you that, for example, drugs are currently not a solution to these problems. But what I propose is: they are going to be. And they had better be because there is no other effective solution poised to work at a societal scale. We just can’t help ourselves. “Just eat the salad and walk every day” simply did not do the trick. We tried. While it works on a mechanistic level, of course, it does not work in practice. Blaming people for their inability to fight their nature is just inhumane and not how we usually progress: we fix reality for ourselves.
While it is not impossible to design a society that is healthier (see: Japan), it’s at such odds with our current culture, and societal change is slow. We should certainly get to work on this decades-long project, but we should also treat this like any other health issue that costs billions of life-years and find a more effective intervention.
The only really effective policy is to inform people that that is the simple, honest truth of every single person, and that the quality of food we eat is important in that equation.
Eat better food, be more active. Yes, it is difficult, especially for us peasants.
But that is science. I hope a miracle drug helps folks preyed upon by the food industry, but side effects of that industry's drugs leave me skeptical of their being lastingly beneficial.
This needs a slight change in wording or clarification, depending on what you meant.
Losing substantial fat when overweight increases your chance of a longer and better quality life than if you had maintained high levels of fat. Losing substantial muscle in that process reduces your chances of the same. It's statistics and never guaranteed.
There is no boogie man trying to scare people away from broccoli.
Consider the type of confounding that occurs in studies of people losing a lot of lean mass: cachexia, restriction to bed, famine.
Traditional weight loss methods have not shown the magnitude of survival benefits wrt cardiovascular disease, joint pain, diabetic complications. Exercise is wonderful, but as a public health intervention it is not sufficient.
If anyone looks at the totality of the high quality GLP1 clinical evidence and concludes these drugs are going to cause a net reduction in longevity and quality of life, then they should step back and assess their process for evaluating information.
It's literally not effective. As in, well-studied, isn't effective.
Again, it's the only guidance one has to go on, personally, so it's fine to hold onto that as an individual navigating the world, but it is emphatically not effective policy.
In hindsight they were exactly right- and they saved at least tens of million of lives by acting quickly[1].
Anyone can put up impressive #s on a leg pres. Try the bench press instead. No one impressed by leg press.
In regard to the oft claim of obese people being stronger or more muscular, not really. Studies show that obese people carry only a tiny extra 'lean body mass' compared to non-obese people when matched for height, age, and gender, and much of this extra mass is organs, not muscle. Otherwise, the extra weight is just water. Sometimes it is even less because obesity impairs movement, leading to muscle loss due to inactivity.
If obese people seem strong it is because the fat reduces the range of movement for certain lifts like the squat and bench press, so it's possible for obese people to put up impressive numbers owing to having to move the weight less distance. Same for pushing movements, e.g. linemen, as being heavier means more kinetic energy, but this is not the same as being stronger in the sense of more muscle output. This is why obese people are not that impressive at arm curls or grip strength relative to weight, but wirey guys can curl a lot relative to weight or have a lot of grip strength. An obvious example of this is overweight women having worse grip strength compared to men; the extra fat does nothing.
However, this study is suggesting that semaglutide causes more muscle loss than would be expected based on calorie change alone, not just that weight loss is accompanied by muscle loss.
A lot of comments seem to be missing this critical part of the study.
I wouldn't be surprised if this doesn't replicate, but what they describe isn't quite what you might assume based on some of the comments in this thread.
But sure, it's not effective but only because people have a hard time fending off our cravings. It requires breaking our cycles and learning how to eat better and eat less and do something other than lay around watching tv.
As to policy: if we curbed the corps' ability to profit off our ill-health, then we'd surely be doing something positive for society. It would also be very helpful to have cleaner air and more and larger parks that are safe for one and all. What can I say, I dream big.
Personally, I recommend everyone avoid any and all refined sugar and alcohol, as they mess with our hormones and gut biome. And that's very difficult for 2024 America, evidently.
That is like dismissing a bug report because "it works fine on my machine", though.
This comes from professional bodybuilding, where people are using steroids, along with various, uh, interesting chemicals on the cut[1]. It has almost no benefit to (real) natural bodybuilders. It's closely tied to cycles of steroids.
[1] Ephedrine, Albuterol, Clenbuterol (literally only approved for horses in the US), DNP, and probably more that I haven't heard of. Here's an NIH article on the dangers of DNP, to put it in perspective: https://pmc.ncbi.nlm.nih.gov/articles/PMC3550200/
Most natural bodybuilders recommend the 'clean bulk' where one simply eats the same cutting foods but in larger proportions. And also not to be too strict in general - that way lies disordered eating, binges, purges etc.
No one is questioning CICO.
The part being questioned is why it's more difficult for others. For example, my wife and I share an almost identical diet and activity level, yet i struggle to keep weight on and she struggles to keep weight off and with similar lifestyles. CICO works of course, but not only do our bodies innately do different things with the calories that they process but we simply experience that world differently.
I could drop down to unhealthily thin levels without even trying. She would be in misery even trying to maintain my weight.
This isn't an excuse necessarily. Rather just saying there's a lot of information beyond simple CICO that we're missing. Complexity in biome, addictive behaviors, and a full on assault from the food industry.
The ease i have in weight loss is not due to my own efforts. Thin people shouldn't break their arm patting themselves on the back, because imo it's usually not due to our own will.
Hunger reduction + supraphysiological muscle gain from steroids and growth hormone - (heart) muscle reduction = win/win?
Heart problems are one (of many) of the main problems these guys face, so I won't be surprised if Ozempic is used to kind of "balance" the effects of other drugs.
And I get that it’s fun but when you’re called out on it you don’t have to get upset. Ten years from now, either you will realize how comical you were being or you will still be the same. It’s better for you if it’s the former. That’s all I’m going to tell you, for your own good.
Without proper control you could also say that weight loss is associated with loss of heart muscle mass.
They actually had an exhibit showing the effects of obesity on tissues. This was before fat acceptance became a thing. That was really an eye opening exhibit showing shrunken muscle tissue, shrunken hearts, shrunken/squeezed lungs, etc.. in obese people.
Kind of opened my eyes as to how crazy the changes are.
The athletes heart is going to beat at 1/2-1/3 the rate at rest compared to the obesity-enlarged heart and a stress test is going to show the athletes upper heart rate limits are much much higher.
It's like a hacker flipping bits in a binary trying to figure out what's going to happen.. except the hacker at least can look up the complete machine code.
It'd be nice if people didn't have to fight their nature. Our society demands we act in ways that are unhealthy and unnatural. We're forced to sit in chairs 8+ hours a day from very young ages. Children have teachers making sure they stay in their seats, and workers have supervisors enforcing inactivity either in person or using webcams and software. Companies like Amazon insist that their employees piss in bottles or wear diapers because leaving their workstation, even to use a bathroom, will get them fired. The demands of our daily lives and the design of our environments keep us from living the way we've evolved to live and it's normal and should be expected that many people will struggle with that reality more than others.
Either our society and environment needs to change, or our biology and chemistry need to change. Turns out, it's easier to change ourselves than it is to change the massive systems designed by greed and exploitation that we're forced to live in. We'll adapt. Today it's with drugs. Tomorrow it may be genetic manipulation.
I disagree, everyone I know who has been on a keto dietic consumes little to no fruits or fiber. Honestly, I'm not sure how they use the bathroom successfully with such little fiber ingestion.
But bodybuilders have been using tricks like these for decades (obviously at much more ridiculously high amounts) that work quite successfully for this exact purpose.
No, not really. Yes, this is how you lose weight, but this is not how you have to be to be a healthy weight.
I'm thin, I don't exercise, and I'm not hungry. I feel great.
I can sit around and jerk myself off about discipline, but the truth is I have none. I have done absolutely nothing to be in this position, it's all luck and factors far beyond my comprehension.
if a drug is able to induce that same feeling in others, I say go for it. It sucks that a normal caloric intake translates to pain, hunger, and constant brain noise for a large segment of the population.
Obesity tends to cause heart enlargement (https://radiopaedia.org/articles/obesity-cardiomyopathy), larger muscles (as you're doing essentially built-in weight training just walking around), and organs don't tend to shink; cross-sections show a pretty similar body cavity (https://www.cultofweird.com/medical/human-body-slices/) - the fat largely goes on top of it.
We should not be talking about losing "losing weight" as a substitute for saying "losing fat," which is what most people mean. Likewise, when people say they want to "gain weight", they almost always mean they want to "gain muscle."
Why does this matter? Trying to manage one's health or fitness as "weight" gives (most) people the wrong idea about what their weight number represents, and what to do to improve their level of fitness and dial in on the anatomically appropriate amount of body fat. As an example, it's possible (although admittedly unlikely) for one to work hard to gain muscle and strength while reducing body fat and stay exactly the same weight the whole time. Their overall health, fitness, and longevity will be significantly improved but pop fitness will tell them that they haven't made any progress at all.
The food is most of it, but it also doesn't help that our environments and society don't allow for as much mobility and exercise as our bodies evolved to expect. You can't force people to sit in a chair for 8-10+ hours a day staring at screens and then be surprised when a bunch of them are unhealthy. It's more profitable if you ignore people's health and keep them in place and working on task without interruption though so here we are.
[1] https://en.wikipedia.org/wiki/%CE%92-Hydroxy_%CE%B2-methylbu...
At some level of fat, which is actually more then "thin", you are perfectly fine. Further weight loss is about aesthetic or athletic performance, but has zero effect on health or even slight negative estimated health effect.
You are correct, fruit is mostly sugar so no fruits. Some keto adherents allow the occasional handful of berries, but I found that just made me unreasonably hungry later on. Not everyone has this reaction, though.
There is plenty of fiber in above-ground vegetables. And even if there wasn't, it's not like eating only meat would kill you, humans evolved on the plains and/or jungles of Africa where meat was almost all that was easily available.
Re fiber, A significant portion of the population (maybe a majority) doesn't need much fiber to use the bathroom. It seems like this need is a common situation that people assume is a universal truth. Further, fiber can lead to constipation for many people.
There is significant heart remodeling after even things like major amputations because of the changing demands on the heart.
Everybody already understands that "losing weight" means losing fat, not muscle. They don't leave the doctors office after a weight warning thinking they need to stop going to the gym.
Likewise, nobody is scared of gaining muscle because they think it will be bad for their health.
Fully 13% of the population lives in an area with restricted access to grocery stores[1]. Couple that with car-centric anti-pedestrian development[2] and you have a definitively societal problem. Addressing that with taxes on the individual will not address these causes, only shift the burden further onto the poor.
1. https://www.aecf.org/blog/communities-with-limited-food-acce...
2. https://www.economist.com/finance-and-economics/2023/11/09/i...
If so, I would be very curious to that reference.
Im hopeful that these drugs can give people a toehold to tackle these deeper issues, and try to emphasize that they are not a panacea.
People are a product of society, and society is a product of people. If we want to live better people will have to change too.
Gotta start somewhere.
This equates to a 300lb male consuming 272g of protein per day. There are 139g of protein in 1lb of chicken breast.
The RDA to prevent deficiency for an average sedentary adult is 0.8 grams per kilogram of body weight. A 300lb male needs about 110g/day at this RDA.
Outside of noob gains it is incredibly difficult for a natural to add muscle mass when in a calorie deficit and recomposition at maintenance calories is also inefficient in the vast majority of cases.
They won't bulk the same way someone on gear does, but it's still the most efficient way to add muscle mass in the vast majority of cases.
I can't figure out how relevant that is. From what I've seen of obese people they always struggle with limited mobility, which often only improves with physiotherapy (or other forms of exercises). Sumo wrestlers are huge but can move faster than an equivalent obese person because (I assume) they have stronger muscles due to their regular regimented training and diet. Does this mean they have more muscle mass than fat compared to an equivalent obese person? Does more muscle mass indicate stronger muscles?
I'm still taking it because it's cheap and I figure I might as well, but anavar is likely significantly more effective.
> Does more muscle mass indicate stronger muscles?
Yes. Strength for specific movements involves CNS adaptation, but if you look at the top tier of powerlifters, ranking them within a weight category by MRI muscle mass would produce basically identical results to their actual rankings.
If you and your wife eat the same diet in the same quantities, it's no surprise she would have a propensity to gain weight and you wouldn't unless she's substanially larger (i.e., taller and/or heavier) than you. Women in general just burn fewer calories for similar sized vs. men. That said, this is ALL population averages. Everyone knows someone who seems to be able to eat literally anything and never gain weight... it likely is just as simple as their metabolism is such that they burn more calories than the average person. Population variation will always lead to some people with outliers both in high expenditure and low expenditure.
Examine has done excellent write ups on all the research related to it, which can be found below. They recently paywalled the bulk of it, but it's still on the wayback.
https://web.archive.org/web/20240310004421/https://examine.c...
Who are these people? I suspect a lot of people who are overweight/obese and taking GLP1 drugs have very little to no concept of proteins role in their body composition. Essentially all a GLP1 drug does is modulate down your hunger (and you get full faster). That does not give you any of the tools or skills to create a diet or exercise plan. Both of those require intentional planning, research, skills, and time. They're definitely 3 separate things.
That's the point though. I'm saying that we burn calories at different rates. We burn fat at different rates. We have different rates of addiction, cravings, etc.
Just saying CICO is the same boring and borderline inaccurate language that has led to nearly zero change in the population at large. may as well just tell them to use physics correctly to lose the weight, because it's the same effective language.
To even determine CICO is fraught with difficulty and inaccuracy in both CI and CO. You can hand make everything, weigh every ingredient, and even then you struggle to determine how much you're CO. At best you'll have an estimated CO but then what do you do when your weight isn't changing? you have to start adjusting the math because clearly you're not burning as much as you think you are.
This is made much, much worse with the fact that we don't actually burn that many calories with exercise. And even with what is burned, the rate of burn changes drastically based on your current weight and how long you've been losing weight.
The fact is, the point is, CICO ignores all the real challenges and thereby all the real problems people need to understand and face.
This does not make any sense. Why would the body prefer anything over the most dense and available calorie store? Protein in muscle gives shit calories per gram, it is hard to build back and generally less available than fat: the number one energy store, doing exactly what it does.
What I don't understand about these drugs is:
Ok, you are taking the medicine to lose weight, but are you eating the same shit as before in the process?
The answer is always "pfft no, I am going to eat healthier"
So why don't you just eat healthier now?
When our ancestors faced famine, it makes sense for the body to shed as much muscle as possible, since this reduces the metabolic rate in the medium-long term.
Muscle is more metabolically active than fat. Although fat can be used up for energy more readily, but muscle takes more energy to maintain. Burning fat just to maintain (unnecessary) muscle doesn't make sense in terms of survival.
I think we'll have to disagree here. At the end of the day CICO is the formula. That obviously doesn't account for the human factor in regards to the adherenace rate, but it does, fully encompass the 'if you were a robot and were fully adherent how do you lose/gain weight' method.
> To even determine CICO is fraught with difficulty and inaccuracy in both CI and CO. You can hand make everything, weigh every ingredient, and even then you struggle to determine how much you're CO. At best you'll have an estimated CO but then what do you do when your weight isn't changing? you have to start adjusting the math because clearly you're not burning as much as you think you are.
I won't say it's 'easy', but it's also not particularly hard either with the multitude of widely available food databases for measuring calories in. As for calories out, it's arguably even simpler: measure your weight every day, take the average across the week, and watch your weight trend week over week. Calories out can be calculated simply by comparing calories in vs. weight lost/gained... and extrapolating. It's simple math, and very effective in my experience.
> This is made much, much worse with the fact that we don't actually burn that many calories with exercise. And even with what is burned, the rate of burn changes drastically based on your current weight and how long you've been losing weight.
Essentially irrelevant if you follow my above suggestion for how to measure calories out. It's just part of the bucket of calories burned, so as long as you're reasonably consistent with the amount of exercise you do then your averaged weight will account for any exercise based caloric expenditure.
C57BL/6 – the canonical inbred fully homozygous mouse that unfortunately is used as the “HeLa cell” of almost all experimental murine biomedical research. I understand the reason this happened, but there is no excuse in 2024 to use just one genome (and an inbred one at that) to test translational relevance.
Consider this work a pilot worth testing in NZO, DBA, A, C3H and BALB strains and some F1 hybrids. Whatever the results they should have good generality to mice in general.
Cadmium in some strains of mice is highly toxic to male testes. But if, as in the C57BL/6J strain, you have a “lucky” transporter mutation, then no problems at all. This kind of variability has been known since the turn A. Garrod in the early 1900s. And ignored by many.
Here is the data on the cadmium example I just mentioned:
https://genenetwork.org/show_trait?trait_id=13035&dataset=BX...
I don't know if these are the best resources, I only gave them a cursory glance. The summary does a good job.
AI Summary (Brave Searc) - Hydrostatic, DEXA, Bod Pod Comparison https://search.brave.com/search?q=hydrostatic+weighing+vs+de...
No, they don't. They simply eat enough to continue muscle growth and attempt to shed fat before a competition. Any non-competitor doing this is just engaging in quasi-religious nonsense or rationalizing a bad diet.
Bulking and cutting have meaning, and we're not going to turn it into any caloric surplus vs deficit.
This is like trying to solve aerodynamics with Newtonian physics only. It’s not useful. CICO ignores the variability of base metabolism.
https://www.youtube.com/watch?v=eCpeRdUkegE can walk you through a handful of the latest studies.
You need to be in a caloric surplus to efficiently build muscle mass regardless of whether or not you're natural. I'm honestly confused how this is even an argument we're having. No one is saying you need to eat in 5000 calorie surplus as a natural, but everyone still refers to the period where you are in a caloric surplus as a bulk and a period where you are in a caloric deficit as a cut. This is not and has never been restricted to people on gear.
Metabolic syndrom is characterised by the basal metabolic rate reducing in response to reduced calorie intake or increased caloric expenditure. In most of us this is good. It gets the immune system to quit mucking around, for instance. In the obese, however, it can sometimes mean their bodies will literally stop doing essential shit before it will concede and begin burning fat. It will then do everything it can to refill those fat cells.
You can model a human thermodynamically. But to my knowledge, this isn't used in medicine because it isn't practical. (I'm saying this, by the way, as someone who can eat anything and laze around and not gain weight because my metabolism is tuned the other way.)
CICO reminds me of something we do in finance: burying the complexity in a magic variable. For CICO, it's the CO. Because if you decompose it into its active and inactive components. Exercise is the former. But the latter absolutely dominates that term.
I used to be you - in most of my 20s, I found it very easy to just eat well, east less, etc. It didn't take any willpower on my part to be fit. It was trivial. I didn't understand why fat people didn't just do the same things I was doing. I thought they had to want to be fat!
Then I got busy with other things, I had less and less free time, fast food, etc. got more and more convenient. Then the pandemic happened and I started just ordering uber eats twice a day. And suddenly I realized "holy shit, I'm fucking fat."
And then I tried to go back to my earlier habits, and it was hard. Things that took zero willpower on my part suddenly meant spending a significant portion of my day fighting different urges.
Was it within my power to do so? Sure, in theory. Everyone, given no other task to do but focus their willpower on just not eating too much, could likely eat healthier and lose weight. But that's not reality, it's difficult, and it ends up slipping down the priority list behind a dozen or two other things.
But on tirzepatide, my relationship with food nearly immediately reverted back to how it was when I was younger.
The fact of the matter is, America has a huge amount of obese people that know they shouldn't be and know in theory that fixing their diet and exercising would resolve their issues. And yet they still are fat. Very very very few of them want to be that way. And the reason is it is hard to just eat healthier when you have that level of food craving
But the issue is all of the studies I have looked at look at total FFM which does include the loss there. If you are on these GLP-1s there is water weight you are going to lose and keep off while on them due to the anti-inflammation effects, etc., and that water weight is going to be part of their calculations of FFM that has been lost.
Was curious about this, went hunting for some rough data, this [0] suggests every kilogram of fat held can be drawn down at ~70 food-calories per day.
So someone with 25% body fat weighting 100kg (~220lb) could draw 1750 food calories per day, which strikes me as pretty ample unless they're also adding a bunch of physical activity.
Also for me if I go to crossfit after workday ends I don't get cravings the rest of that day. If anything I want to go to sleep instead of eating candy in front of the TV.
https://faseb.onlinelibrary.wiley.com/doi/epdf/10.1096/fj.13...
https://faseb.onlinelibrary.wiley.com/doi/epdf/10.1096/fj.14...
https://www.sciencedirect.com/science/article/pii/S216183132...
https://www.mdpi.com/2072-6643/12/8/2457
For weight lifting helping decrease this: https://www.mdpi.com/2072-6643/11/11/2824
https://journals.physiology.org/doi/full/10.1152/japplphysio...
https://link.springer.com/article/10.1007/s00726-013-1506-0
https://journals.physiology.org/doi/full/10.1152/ajpendo.005...
https://onlinelibrary.wiley.com/doi/abs/10.1002/mus.21780
https://journals.physiology.org/doi/full/10.1152/ajpregu.004...
https://www.mdpi.com/2072-6643/10/4/423
These are just a tiny subset of the studies done - google scholar can find you many dozens more, if you desire. And, of course, the fact that these studies exist it all necessarily implies that you lose muscle mass when in energy deficit, as you will see in the control groups for them.
It seems likely we've evolved to reduce energy expenditure in other ways when we regularly induce physical activity, too. Walk 20,000 steps or spend a couple of hours on the treadmill? Your body finds ways to reduce your energy expenditure elsewhere.
I’m sure there’s some people that this might apply to, but I suspect it’s a much (much) smaller subset than people that are actually obese. For the rest, just decrease your intake until you lose weight. Not much else.
> You can model a human thermodynamically. But to my knowledge, this isn't used in medicine because it isn't practical. (I'm saying this, by the way, as someone who can eat anything and laze around and not gain weight because my metabolism is tuned the other way.)
Exactly what variables are missing then? We can agree that exercise, although certainly burns some calories, is not really the lever you want to pull if you actually want to lose weight by itself. What other variable besides changing how much food you eat would you suggest?
It's not a profound statement to say if you starve in a desert you'll lose weight. The question is how we can apply this to real, normal people. Or if it's even possible in a food-weaponized world.
My view is that we're in the realm of addiction more so than simply answering "how" they mechanically lose weight. This is a public health crisis, one we need to be open to exploring.
75% of the calories in broccoli is from carbs, sure, but because the overall calorie content of broccoli is so low, it's still considered low carb.
https://www.nutritionix.com/food/broccoli/1-cup
A 1-cup, 156-gram serving is 55 calories, 11g carbs, and 5g fiber, so is only 6g of net carbs for keto purposes.
Should we do more research to find if anything anything specific that may be causing overeating or food non-satiety? Sure. Is the answer likely to be something that is essentially 'tastier food is easier to overeat, and tastier food is much more available than it used to be'? I suspect that is the likely conclusion.
I think GLP1 agonists are a great tool to be used to create that so-called 'willpower' to stop overeating (or, an easy way to reduce food noise, whatever you want to call it). The next step is figuring out how, as a society, we make it easier for folks to make that lifestyle change without a constant stream of 'willpower drugs' for the rest of their life.
While some YouTubers may be correct about the things they talk about, or may even be doctors or researchers, I think we're in a pretty sus world if disputes about factual or even anecdotal information can come down to whether someone's watching and getting recommended the same content on a video site designed to exploit chronic viewing habits.
If your crowd does differently, just cite that, if they don't, speak from a place of speculation if that's what you'd like like them to do, because that's basically what watching YouTube does for a person.
I think if I were taking Ozempic I would ask my doctor to halve the rate of progression to higher doses to make the whole process easier to manage, not just managing muscle loss but also the whole of life impact. The official protocol is very "crash diet" in style.
Anyone thinking of taking Ozempic should be aware that many people abandon the drug within the first two years, due to too much nausea, diarrhoea and cost.
Yes, and again - as i said previously. No one is questioning if CICO works. That's like if questioning if physics works. No one is doing that. The laws of the universe are still intact. Talking about humans is the constructive conversion most people are having.
But yes, he is also popular on youtube.
Other people are, in fact, questioning CICO. Look at the other commenter talking about base metabolism changes.
To put an analogy to this: Gambling addicts often lose lots of money at casinos. The behaviors that lead to them being addicted to gambling are in many ways likely equivalent to overeating problems. Nobody asks 'why are gambling addicts losing money?' because we know the reason (casinos have the house edge... you always lose on aggregate). And yet, with food, people consistently ask the question 'why are people so obese?' as if the answer isn't very obvious: they're eating too much food. It's purely as simple as that. The behaviors that lead to eating too much aren't nearly as focused on, in my opinion. Much time is spent on 'the kinds of foods eaten' and how specific things are bad for you, which is essentially like arguing that people should play more blackjack and less roulette or something.
I disagree. CICO is fundamental physics. Just because metabolism changes does not mean you can produce more energy than you take in. CICO always applies, and it's so 'duh' that it's nearly pointless to discuss in my mind.
Their points about metabolism changes is that the details matter. Finding a way to break the cycle will yield more gains with the population than telling people to starve in a desert.
I also like a bunch of other channels and have derived what feels like good information from them, I'd recommend them on that basis to people I felt would find it useful or entertaining. Just because I wouldn't cite them as an authoritative source doesn't mean it's a strike against them, it just means I don't think it's fair to tell someone they're wrong because my favorite YouTuber, even if they seem credible, well-natured, and are worth recommending, says X.
There are plenty out there doing good by their viewers and I love that, especially Canadian ones, but it's insufficient for being hyperbolic, imo, about what's impossible to make a claim about, and I don't think arguments from apparent authority are to be encouraged anyway.
In some cases, I've checked the advice of other MD content producers against real practitioners, and they've gave me the thumbs up in terms of credibility, and that obviously changes the vibe a bit, but still I'd hesitate to go too far with that, there's a lot people will do for money and attention.
https://www.chicago.gov/city/en/depts/mayor/press_room/press...
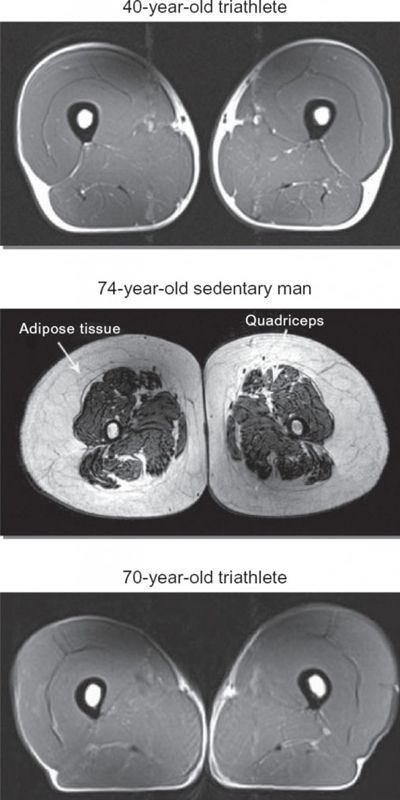{kind=link}