Man I thought we were getting raked with our 8% increase. 75% is unbelievable.
The job-based insurance system in USA is so bogus.
I was on the exchanges, unsubsidized, until this year. Last year's premium went from $3,000/month to $3,600/month. I had to buckle and get on a company plan with less coverage this year.
Meanwhile, every other piece of spare real estate in town is a new medical facility. Urgent cares, palatial orthopedic facilities… There's a crash coming.
If I understand this correctly, enhanced premium tax credits were extended to 400% federal income poverty level during COVID. (e.g: federal income poverty line for a household of 1 is 15k), right?
There is something very wrong with American attitudes.
If you remove one of legs of the stool, the market becomes unstable and you see price spirals like this.
Jonathan Gruber (MIT econ professor, and one of the designers of the Affordable Care Act) gave a fairly detailed talk about how and why they designed the ACA the way they did, learning from a similar law in Massachusetts: https://youtu.be/2fTHqARiV_Q?si=SRC6Np-rjgUgAe4Z&t=679
https://www.kff.org/report-section/ehbs-2023-section-1-cost-...
Figure 1.12 shows average annual premiums from 1999 to 2023. The ACA was passed in the middle of that range. It's a sustained upwards march, before and after its passage.
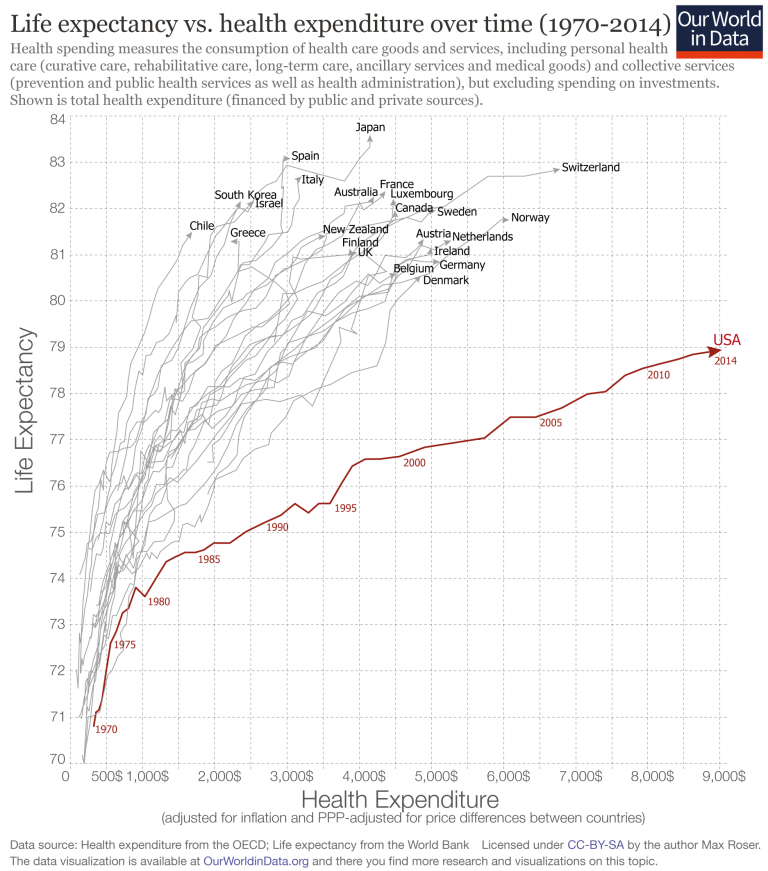
For all that cost - 2-3x as much as the other OECD nations spend, inclusive of taxes - we get shitty outcomes.
https://assets.ourworldindata.org/uploads/2016/04/ftotHealth...
Encourage not sleeping, advertise and manufacture processed garbage, encourage drinking poison, and most of all encourage working long hours over getting any physical activity.
Yeah, good luck with that. It’s an every man for themselves environment, the government and American society is fine with throwing your body into the meat grinder for more profit.
Ironically we’d be much more productive if we incentivized a healthier lifestyle for the population.
Mitt Romney took the plan from the Heritage foundation (yes, the conservative neocon think tank). Hard low-controls capitalist plan.
Heritage foundation made this plan after Hillary Clinton pushed universal healthcare in 1994, as first lady. Howls of 'death panels' were heard all over republican talking points and radio shows.
(The 'death panels' aka rationing was seen as bad for government to do. However, we see a new type of rationing, based upon how much patients cost, and then denying care. That lead to the UHC execution, then approving more procedures, then getting sued by shareholders for that. Personally, government death panels are preferred to capitalist death panels.)
Put simply: Obama passed republican legislation put forth by a republican governor and a republican thinktank, and was deemed a socialist. And now, the program is basically destroyed.
Prices are rough these days, because Republicans later removed the individual mandate. The system was never gonna survive that; it changes the economics entirely.
It even shows up in poll data. This poll from Oct 2024 shows a 15 point difference when the wording changes. +34 favorable when asked how people feel about the ACA, but only +19 favorable when asked how they feel about Obamacare.
https://navigatorresearch.org/the-affordable-care-act-remain...
Labeling the ACA as Obamacare was an incredibly effective tactic to leverage the American public's racist tendencies against the public's own interests.
Consolidation of hospitals/medical facilities/practices and the rapid spread of PE firms is absolutely destroying our already cracking healthcare industry. A crash is definitely coming. And just like with the financial crisis, we’re going to be the ones footing the bill and/or just dying on hospital steps.
Combined with so many doctors fleeing states with strict abortion/anti-LGBT laws, as well as the dismantling of programs encouraging doctors to work in under-served (often rural/low income/isolated) areas, it doesn’t take a genius to figure out who’s going to be hit the hardest.
My mother is an elementary school teacher in a conservative Michigan town. She generally doesn't talk politics at work, but a coworker mentioned that the school's "no questions asked" free breakfast and lunch policy was ending next year due to federal education cuts. My mom's co-teacher, who voted for Trump, expressed surprise, saying she didn't realize that was something likely to be cut, or that the states would make up the shortfall.
Anyone remotely following US politics wouldn't be surprised, and would know that most states are fairly strapped for cash. (Whether that's societally optimal is besides the point.) This is a pattern I see over and over again, on both sides of the line: you see Trump voters surprised that cuts to the FDA result in higher food recalls, and you see Democratic voters saying that nothing got done over the last four years.
It baffles me. I have more awareness of the local politics in our small Canadian town than I did when I lived in Chicago, and it all just comes from listening to my friends talk about current events. It's a wild feeling.
Premiums for all plans have been going up basically every year, even for those who don't qualify for any subsidies.
Today for most employees a HDHP is the ONLY option, and the cost is much higher than the old standard health plans were.
That's a large reason why there is no major change in this area, even though one is sorely needed.
Personally, I'd just open Medicare up to anyone who wants it by paying some additional fee each month and see how that goes, but that's too simple for most politicians I think.
It wasn't "destroyed" because it was "deemed socialist". It was destroyed because it used tricks of law to get something that didn't have broad enough support at the time done and those regulatory tricks were not durable. Same exact story as Roe v Wade but in a much more compressed timeline.
Unfortunately, the whole debacle has likely hardened the resolve of everyone who is against it even though a functional Romneycare system would likely be satisfactory to them (and needless to say an improvement over the status quo).
Turns out "the perfect is the enemy of the good, ship it" isn't how you run a society. This is a common theme. Stuff that's 50-50 either gets gutted or repealed with time. Something needs to be truly popular, like will lose you votes if you undo it, in order to stick around. For example no amount of pothead deadbeats or drunken wife beating is bringing weed or alcohol prohibition back at the state level.
We're 15yr on from the ACA and with very few exceptions things are worse. The nation likely would have been better served by letting the states that were inclined to run such systems continue doing so without federal meddling.
You're getting fucked (as am I!), but the ACA isn't what's doing it.
Then, once it fails, they will just lie and again blame Democrats for it instead of circling back to their talking points about how they wanted to kill Obamacare.
This is just some people. I have met a fair number of people who just think it is too bad, so sad if you are too poor or do not have a good enough job for good healthcare. I was visiting Canada once, and the folks at the company I was visiting recounted the last American who rolled through who espoused the "well, I guess they die" talking points - to their horror.
That's an understatement on the order of saying WW2 was a rebalancing of geopolitical power.
Healthcare is what? 20% of GPD. Likely half of that is paper pushing compliance checking rubber stamping that likely ought not to exist.
People may think they're paying full price because they make some monthly premium payment... which isn't true, as either the government subsidizes a portion of the premium, or you're getting group rates that are way cheaper than if you tried to buy insurance on your own. So even "full price" is receiving a form of subsidization through the operation of the program.
The disconnect is that the media and politicians talk about Obamacare like it's this free healthcare giveaway, so people who pay anything assume they're not on it. They could literally be using the ACA marketplace with 0 understanding that it's "Obamacare". Most people just perceive ACA as government overreach into healthcare, not realizing they're benefiting.
I'm sure it's by design.
But so so so much is wrong financially for hospitals, clinics and pharmacies.
This administration is poking the house of cards with a really large stick.
Pharmacies are so fucked by PBMs( that politicians only pay lip service to dealing with) that they _owe_ money to the PBM everytime they fill many prescriptions. Negative reimbursements. Many small time pharmacies now play games to refuse prescriptions because of how bad it is. PBMs have tried to counter by having distributors write contracts that bar refusals. Chain pharmacies aren't doing much better and are where the negative reimbursement customers end up.
"Mom & pop" doctor offices simply are going extinct. Due to both polticians lumping on requirements for digital records, infinite insurance games and cost of real estate going to the moon, every new doctor just joins a mega-hospital-network because they are already 2 million in debt after schooling. Old doctors just sell out their clinics to those hospital networks. Suddenly doctors that work there get put under strict quotas. This is something I've seen happen in real time in my suburban part of NY. My doctor's office that also fell under the growing blob of a mega-network, now has numerous signs saying "new concerns brought up during the appointment must be done under a new appointment for billing purposes".
Your insured pool now includes people who don't take care of themselves and treat the emergency room like a private doctor's office.
Other countries with government-controlled healthcare introduced wait times to encourage people to consider whether eating that extra donut was worth the health risk. I suspect we'll follow that path, too.
I want to know details of your situation, because my exchange premiums are like $300/month.
> For generations, members of the Beers family of Canton, Ohio, have used Christian faith to sell health coverage to more than a hundred thousand people like Martin. Instead they delivered pain, debt and financial ruin, according to an investigation by ProPublica based on leaked internal documents, land records, court files and interviews. They have done this not once but twice and have faced few consequences.
Even the legit ones don't have to cover stuff; they aren't health insurance. Even if they do, many facilities and docs won't take it, because they aren't required to cover things and they don't want the fight.
Also it's technically Romneycare. The political right got everything it wanted with it, similarly to when Nixon passed HMO funding that tied insurance to work, basically forcing a work requirement in order to get healthcare:
https://en.wikipedia.org/wiki/Health_Maintenance_Organizatio...
This might be the biggest thing that caused US healthcare to double in cost vs the rest of the developed world, which provides universal or single payer healthcare to their citizens for free or nearly free.
Also the article got the numbers wrong. To be accurate, they should have said $400 or more, roughly $5000 per year for working adults pushing 40. More for families. That was 10 years ago when I was applying, I'm sure it's more now.
I'm surprised that a startup isn't providing transportation for medical tourism. A friend of mine lived in Costa Rica for a while decades ago, and care was covered even for noncitizens. So a round trip ticket and living abroad for weeks would still be cheaper than insurance plus deductible here.
It's to the point where half of you will block nationalized healthcare for the other half, even though we would continue paying double to cover you for free too. So much for objectivism.
Edit: I forgot my point, which is that I believe that healthcare may be a natural monopoly, which is when something that everyone needs must be regulated, or else it becomes a monopoly where the vendor charges as much as possible because people have no choice:
https://en.wikipedia.org/wiki/Natural_monopoly
Other examples include electricity, water, sewer, trash and probably education.
> If healthy people opt out, the insurance pool is left with those who cost insurance companies more — people who can't go without health insurance because of chronic conditions or expensive medications. "That's why insurance companies are going ahead and charging a higher premium, with the expectation that the market is going to get sicker next year
IMO participating on HN is a privilege earned through good faith discussion over time. If they want to make a point they can do it without being smart aleck and wasting peoples' time.
The short term effect would be an increase in costs but no increase in pay for most people.
It's a weird scenario. American politics is so loud and omnipresent that I, as a Brit on the Internet, end up following it involuntarily because it ends up in every discussion everywhere. But so much of it is just weird things made up by right wing talking heads.
Edit:
In the context of this topic and the near term, this looks like blue states implementing universal healthcare, and letting red states figure it out themselves (considering how dependent red states are on the federal government [1] [2]); Oregon is up first [3]. You can increase state taxes to fund this, reducing tax dollars sent to the federal government, if properly engineered.
[1]. https://time.com/7222411/blue-states-are-bailing-out-red-sta...
[2] https://usafacts.org/articles/which-states-contribute-the-mo...
[3] https://www.hcfawa.org/oregon_s_path_to_universal_health_car...
22 % Social Security
14 % Net Interest
14 % Medicare
13 % Health
13 % National Defense
10 % Income Security
5 % Veterans Benefits and Services
2 % Education, Training, Employment, and Social Services
2 % Transportation
1 % Natural Resources and Environment
3 % Other
Reagan was the one who brought socialized health care to America. He passed a law saying that hospitals couldn't refuse emergency treatment due to inability to pay. So uninsured people wait until their conditions are bad enough to be considered an emergency, and then show up at the ER. So hospitals have to jack up their rates for everybody to cover the cost of emergency treatment of the uninsured. Expensive treatment that would likely be much cheaper if treated before it became an emergency.
So this Trump move won't save you money, it just changes how you pay.
Instance #234535 of "the bar is never too high for Democrats and never too low for Republicans."
Although only Republicans are in favour of the final option.
They got it from the approximately half of society that they could pander to by saying "look, we did that, vote for me and I'll take it even farther" at the next cycle.
The ACA is going to go down in history as something that caused some yet unknown number of decades of suffering because it was just barely too much just barely too soon. If they'd have kept it in their pants another decade or maybe even less, or legislated a more incremental solution at the time we'd probably be 5yr into something workable by now.
https://www.irs.gov/affordable-care-act/form-w-2-reporting-o...
> The Affordable Care Act requires employers to report the cost of coverage under an employer-sponsored group health plan. Reporting the cost of health care coverage on the Form W-2 does not mean that the coverage is taxable. The value of the employer’s excludable contribution to health coverage continues to be excludable from an employee's income, and it is not taxable. This reporting is for informational purposes only and will provide employees useful and comparable consumer information on the cost of their health care coverage.
So, it went from "I pay $50/month for healthcare" to "my paycheck says they're taking $2k/month! what the fuck?!" in folks' minds.
This is not at all new. It's how every other market operates.
For healthcare, which is not a normal market by any means, it might make sense to approach rationing differently because most people refuse to accept that rationing occurs at all, but cost will always be part of the picture.
I keep saying, cause its true: this is a republican plan, pushed by republican governor, and by a republican thinktank, branded as socialist because a black democrat had the audacity to push it.
The quality of care, technology, and expertise are top-tier for those with excellent insurance or deep pockets. But the system is neither free nor particularly efficient. For many, access is limited by cost, bureaucracy, and inequities. So yes, it is best care available, but not best care accessible.
It's targeted across all US demographics. Sometimes covertly.
And increasingly it's fine-tuned towards individual interests and psychological triggers.
The unsubsidized cost of a standard PPO plan for a family can easily reach $3000 a month. This is situation normal, people just don't see it because their employer is responsible for the cost.
It's also worth noting that the percentages are substantially higher than the averages for the portion of the population who generally votes.
The Biden administration started to heavily subsidized some health care plans with Covid as the backdrop, and now those temporary measures are ending.
In so far as I have found and I might be wrong, congress never voted to fund and subsidize those medical plans indefinitely.
Now health insurance companies are raising their rates on those specific plans since the government is no longer partially funding it, or perhaps not funding them as much.
Then I am convinced the insurance companies raised their rates more then strictly required as they nearly always to to make even more money.
https://www.census.gov/library/publications/2024/demo/p60-28...
More:
https://www.unionhealthcareinsight.com/post/why-employer-hea...
We're talking about folks who non-ironically walk around with signs saying "keep government out of my medicare". https://archive.nytimes.com/krugman.blogs.nytimes.com/2011/0...
> 44 percent of Social Security recipients, and 40 percent of Medicare recipients, believe that they don’t benefit from any government social program.
No, they have wait times. Just like the US does.
https://www.statista.com/chart/33079/average-waiting-times-f...
"According to a recent study by the Consumer Choice Center, the average wait for a GP appointment in the United States in 2023 was around three weeks, two to ten times longer than in Europe. For example, in that year, the average waiting time for a medical consultation was two days in Switzerland, six days in France and ten days in the United Kingdom and Italy."
Five other comments that answered your question. Go on, engage honestly.
Welcome to Hacker News.
Insurance company covers person.
Person gets chronic ill, with covered disease.
Person is now 'less profit' or a cost.
Company, against contract, refuses to cover medication/procedures.
Company waits out patient to die.
The person is demonstrably wronged, but these companies can just wait sick people out. And that's precisely what happened with UHC. You know, Delay Deny Defend.
The risk here will be sick people (and their high costs) moving. As with how Chicago's illegal gun problems mostly come from Indiana.
I'll see your anecdote with another anecdote. Around where I live, for the past few years there was a sudden massive ad campaign for a new orthopedist complete with billboards featuring the presumably founding doctor's smiling face, and various other print and sponsored ads. Their main building is a giant gaudy marble, glass and brass clad building, but there are others that have taken up more mundane buildings. I don't know how such a business launches so quickly with so much $$, but it must be PE. They've certainly got a lot of debts to pay off now, and I can imagine the assembly-line level of care with more focus on low-margin patient satisfaction, encouraging reviews about how nice and friendly everyone was, rather than actual effective care. This is of course my cynical uninformed take after seeing mucho $$ spent on advertising. Maybe they are actually great and effective doctors, for all I know.
If you payed $60 a month you were mega subsidized. I'm at about $500 a month (50s, single, bronze). There's no way I'm suddenly going to be around $900. This is either clickbait or a NPR scare tactic.
Does residency fraud exist? I'm sure of it. Despite the UC and CSU systems not publishing residency fraud statistics, such fraud is universally described as being extremely difficult to execute. I cannot overstate this point. Students routinely depict residency fraud as being more difficult to do than simply paying out of state tuition. The high cost of committing residency fraud makes cancels out any expected payoff. Furthermore, most instances of detected fraud appear to be technical and clerical errors, not intentional deception.
What are in-state residency requirements, and how difficult is the requirement? Evidence for residency includes:
- Obtaining a California driver’s license or ID card
- California vehicle registration
- California voter registration
- California state tax returns
- California bank accounts
- Employment in California
- Lease, mortgage, or property ownership in California
- Severing residential ties to your former state (e.g., closing out-of-state bank accounts, surrendering non-CA licenses)
Additionally, one year and one day of residency is commonly the required threshold to qualify for in-state tuition.
The question becomes, is this effective enough at reducing fraud rather than can fraud be eliminated. I'm sure, like with any system, fraud detection and remediation are part of the operating costs and measured in terms of recovery rate/rate of return - the KPI we're discussing.
A switch from employer-pay to government-pay should be a no-op for employees with employer health insurance. But in a naive scheme, it isn't. The burden for paying for health insurance moves from the employer to the employee (through increased taxes). The employer benefits because they stop paying for health insurance, the employee pays the costs.
Voters, who are mostly employees, would hate it.
OTOH, an on-paper pay raise for employees that doesn't cost the employer anything? That'll be much more politically palatable. "Both your taxes and your salary go up 10%" is a lot more palatable than "Your taxes go up 10%".
For sobering data, check out the link below and look what happened in just 20 years. Unfortunately it stops at 2013, it's probably a solid orange blob today...
People genuinely moving to California would presumably pay out of state healthcare fees until their residency was established. Don't you agree that these fees could be set in a way that served as a barrier to doing what you suggest?
Is there a case that isn't covered by this that you're thinking about?
1. Cal. Code Regs. Tit. 5, § 54022 - Physical Presence. "Physical presence within the state solely for educational purposes does not constitute establishing California residence regardless of the length of that presence." https://www.law.cornell.edu/regulations/california/5-CCR-540...
Sick people are allowed to like California's weather enough to move there. The ADA would also apply when trying to restrict residency in a way it would not for education.
I pay taxes (>$100k/year total state and federal tax burden), I support universal healthcare, and I am willing to pay more for everyone to be covered.
That calculus gets a little different for some folks if the move comes with subsidized universal healthcare and better social services.
> Those who voted for this and don't believe in subsidized healthcare should stay where they are, as I presume they believe universal or subsidized healthcare is "socialism" they don't want.
We agree, but "The Only Moral Abortion is My Abortion" rule applies. https://joycearthur.com/abortion/the-only-moral-abortion-is-...
Perfectly fine. They shall pay out of state rates until they meet the threshold.
> The ADA would also apply when trying to restrict residency in a way it would not for education.
Can you elaborate? In the best case, it's difficult to predict how courts would rule on this. Any relevant case law? Legislation?
I'm not arguing they'll move and obtain residency on day one. I'm arguing it may still make sense to move, pay out of pocket for the 366 days, and gain residency for some folks.
The ADA's Title II would seem to forbid "you can't be a resident, ever, if you've got expensive healthcare costs" sort of rules at the state level, yes? That would clearly not be equal treatment for people with medical disabilities.
Of course if you dig you will find problems, it’s far from perfect. However, the fact that what is collectively outside the realm of partisan politics is not decided by two partners who need to agree is what’s important here. There is a collective tradition. With our judicial system able to give binding decisions on unwritten parliamentary traditions, you even have legal protection for nonpartisan politics.
The US system counted way too much on the kindness of political adversaries. You need to find a new way to do politics, because American conservatives have decided that they will abandon democracy rather than give up power.
It's trivial to construct a threshold and out of state pay structure which cancels this case out. What number of days and out of state pay structure do you feel would cover these cases? How many of these cases do you suspect will occur annually and what is the projected cost? It's a relatively easy problem to solve once we get down to the specifics.
> "you can't be a resident, ever, if you've got expensive healthcare costs"
Great! I'm not arguing for "ever". I think we're in the clear here.
Edit: Let's estimate the volume of this effect using migration after Medicad expansion as a proxy. Over 10 years (2009 to 2019) we find 56,659 interstate moves after Medicaid enrollment growth[1]. In other words, 0.23 percentage points greater annual population growth in the target population. Another study found an in-migration rate(to CA) of 1.4% for medicaid recipients. Being generous and taking the higher of the two, and multiplying it by California's net immigration of 500,000–600,000 annually, gives us an estimated 7000-8400 medicaid migrants a year a fraction of which are migrating primarily for medical purposes. What would you estimate the annual medical expenditures for this group would be and if an "new arrivals" insurance pool was formed, what would the marginal monthly premium cost be to its members?
I estimate that a CA new arrivals insurance pool would have $4B in annual disbursements, and $4-20M in annual residency fraud. Using averages, we can estimate a monthly premium for this group would be about $667/month.
This is roughly on par with unsubsidized ACA premiums for adults in many states. For comparison, ACA benchmark premiums for a 40-year-old in California in 2024 are about $450–$600/month.
It’s exhausting being dragged by low empathy unsophisticated humans frankly, I am personally over it. I was naive about human nature, hard lessons learned.
Compare that to Swisslife, my previous private healthcare insurance: for every 100€ I gave them, 66-72€ were paid to insure in need while I had them. Of course the mandatory dividends were pretty high before COVID, and reinvestment/marketing/sales has to take a bite of that, so perhaps only half of the 30% they take from customers are admin costs, but still, I'd rather give more to my country national healthcare if I could.
Probably the variance you have could be caused by non-admin costs being counted as admin costs.
Last estimates from a few weeks ago were ~$500/mo premiums for a bronze plan (+ deductible of course).
"The expiration of the enhanced [premium] tax credits is expected to cause ACA enrollees’ out-of-pocket premium payments to increase by over 75% on average, with people in some states seeing their payments more than double on average."
"The enhanced premium tax credits were originally passed by Congress in the American Rescue Plan Act (ARPA) and extended under the Inflation Reduction Act (IRA), but they are set to expire at the end of 2025."
[1] https://www.kff.org/policy-watch/how-will-the-2025-budget-re...
I'm not exactly holding my breath that they'll suddenly grow a brain to connect cause and effect against the word of Dear Supreme God King.
I am resourced (out of luck), but also high empathy and intimately familiar with the struggles you mention. The bet isn't only because I can afford it, but because I am so familiar with the data I know I'm right. This is why I am for universal healthcare, see no other path forward, and I hope this better explains the mental model my arguments in this context are based upon.
Of course, this is so heinous that Ronald Reagan outlawed it and there's zero discussion of repealing that law. We've had universal health care in the US since 1986. All subsequent debate has merely been about how it should be done.
These people aren't stupid - far from it! I work with electricians all day and they're sharp as tacks. But most of 'em have been lied to so long they buy it all, hook, line, and sinker. Quite a few of them get drawn in by the social conservative outlook and then just go along with the rest of it.
I mean, same position here. I just don't have $10k to sit in escrow for years. I've similarly got plenty of first-hand experience; one on Medicare and one on Medicaid in the family due to disability, and even with those and a reasonably well paying job we'd absolutely consider moving for a program as described.
Data-wise, we've already got quite a bit demonstrating that California's better-than-average social services are more attractive to homeless folks, to the point where they have ~25% of the country's population of them.
I'm also for universal healthcare. I just don't think doing it unilaterally at the state-level is likely to work very well with freedom of movement between states, as with gun control.
That article purports to disprove the idea that the ACA is based on their proposal, but it actually does a good job proving it.
Most Americans can get pretty good care. It also tends to be painful to get. You don't just go to the doctor. You visit some horrible web site clearly built by someone who doesn't have to use it, go through the list of in-network providers, pick one, call, find out that the list is out of date and they don't accept your insurance.... And then come the surprise bills. The office coded your lab work wrong so it doesn't count as preventive, pay up, or spend an hour on the phone correcting it. You offhandedly told the doctor you're feeling tired lately during your annual physical, and they give you some tips on getting better sleep. Then you get a bill because that counts as a consultation for a specific medical problem, so your free annual physical now requires you to pay a copay.
God forbid you have a major incident. Nobody can ever tell you how much things will cost. You'll be dealing with bills for months, and you won't be able to trust that any of them are legitimate.
The actual health providers are usually OK. The health insurance is godawful.
Is there any evidence that universal healthcare would address the facility and physician shortages in rural areas? It won't make much difference if you give people coverage if they still can't exercise that coverage, or just get subpar care in many rural facilities. It seems that many rural hospitals have turned into glorified helipads to transport many patients to bigger cities.
For example, the uninsurance rate for urban vs rural is only 1-2%. It seems like that wouldn't explain the larger gaps in health outcomes. It seemsbother factors would be more important.
Maybe they're differentiating their care providers and insurer, but that's a level of critical thinking I wouldn't expect.
https://www.nbcnews.com/news/us-news/rural-hospital-closings...
https://www.nber.org/papers/w26182
https://pmc.ncbi.nlm.nih.gov/articles/PMC9633454/
https://ruralhospitals.chqpr.org/
https://www.aha.org/fact-sheets/2025-06-13-rural-hospitals-r...
https://www.kiplinger.com/taxes/medicaid-cuts-and-your-local...
The big question is how big the fee is. Even with Medicare you have plenty of costs, and that's after paying 5.6% of pay into the system for 30+ years. My guess would be that the cost will be similar to what we're seeing on the ACA market with $500-3000 premiums depending on your deductible.
The problem is it costs what it costs. To reduce individual cost you have to reduce the cost of service or pay for it from some other source.
The question was about some universal system preventing rural deaths. If the coverage difference is only 1-2%, then coverage doesn't seem to be the driver. If it's a provider and facility shortage, then we would need some strategy to address the provider shortage, even if we assume we can fix the facility issue by providing higher reimbursement rates or grants.
{kind=link}